3 must-know, never-miss conditions:
- ILO (inducible laryngeal obstruction)
- Large airway collapse with symptoms (LACS)
- Subglottic stenosis
- Christopher, Kent L., et al. “Vocal-cord dysfunction presenting as asthma.” New England Journal of Medicine 308.26 (1983): 1566-1570.
This paper from the archives shows that vocal cord dysfunction has been recognised for a long time. However, it uses problematic languages, and places a firm emphasis on psychiatric diagnoses and conversion disorder as the cause. On a positive note, patients had good outcomes following speech and language therapy.
The classic appearance is anterior closure, with a posterior chink. The is rarely seen but the same clinical problems occur with less dramatic examples, with abnormal movements and stridor. Is ‘brittle asthma’ largely VCD? Glottic closure can cause a sudden PEFR drop. PEFR is dependant on how much air you can get in before you perform a forced expiration. PEFR is unfortunately a waste of time diagnostically.
- Morris, Michael J., and Kent L. Christopher. “Diagnostic criteria for the classification of vocal cord dysfunction.” Chest138.5 (2010): 1213-1223.
Thankfully, perjorative historical terminology is now decreasing. ILO is now the favoured terminology – it is a physiological description of the problem and much more appropriate.
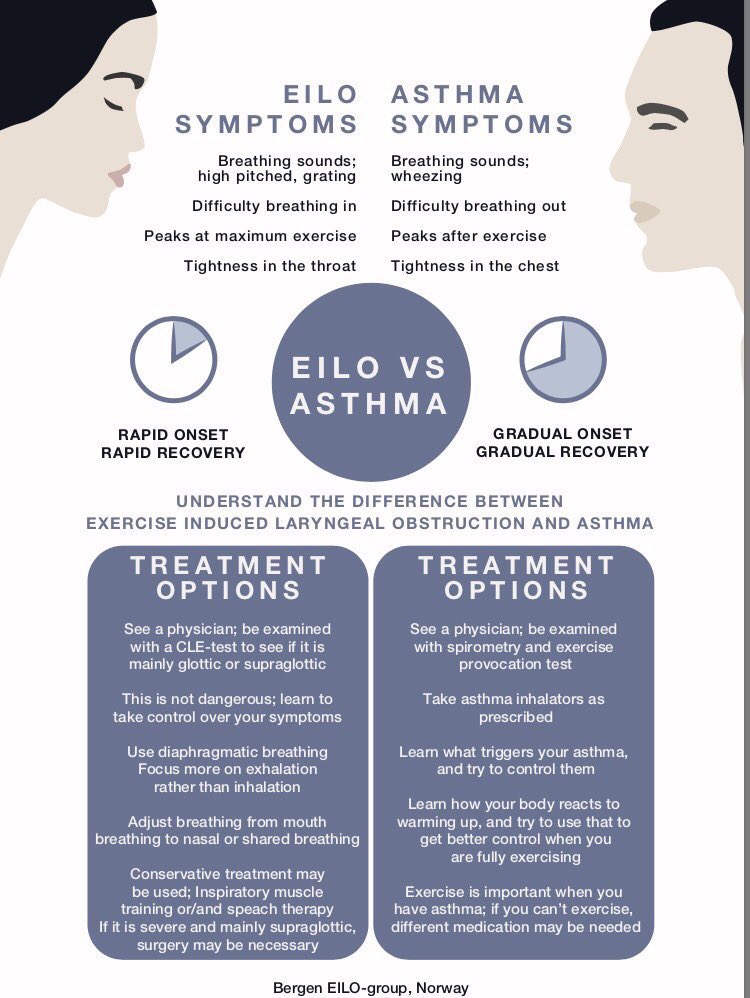
It is important to distinguish EILO (exercise-induced laryngeal obstruction) from EIB (exercise induced bronchoconstriction). 8-10% of all adolescents may have EILO as at peak exercise they get wheeze. It is also possible to have inducible laryngeal obstruction not linked to exercise. An odour e.g. when exposed to perfume on the tube. Direct provocation can clinch the diagnosis.
- Traister, Russell S., et al. “A novel scoring system to distinguish vocal cord dysfunction from asthma.” The Journal of Allergy and Clinical Immunology: In Practice 2.1 (2014): 65-69.
The Pittsburgh VCD index is useful for screening patients for VCD. Remember, it is often a co-morbid condition – there is overlap between severe asthma and upper airway disorder. Therefore don’t cross off their asthma treatment straight away – de-escalate after therapy started.
Find out more at: http://www.laryngealobstruction.com/
Large Airway Collapse with symptoms (LACS) is the preferred current terminology for this group of conditions.
It includes excessive dynamic airway collapse (EDAC), which is often a benign phenomenon due to pressure changes and affects the posterior trachea. It may not be responsible for symptoms so don’t rush to operate/stent. Treatments are mainly physical therapy, cough assists, mucolytics +/- positive pressure support (CPAP). Portable CPAP may be an option – we expect a trial report soon. Early signals are it increases walking distance but it is not acceptable to patients to use in longterm. Relapsing polychondritis is a rare cause. ‘EDACS cough’ is a large airway centred problem, often associated with high BMI.
Tracheobronchomalacia can affect the anterior or lateral trachea and is a cartilaginous problem.
- Kalra A, Abouzgheib W, Gajera M, Palaniswamy C, Puri N, Dellinger RP. Dynamic airway collapse for the internist: New nomenclature or different entity? Postgrad Med J. 2011 Jul;87(1029):482-6.
In subglottic stenosis inspiratory flow may be as low as 10% predicted. There is an audible wheeze. We often see attenuation of inspiratory flow and less attenuation of the expiratory phase of the flow volume loop. This is not VCD as wheeze is there all the time including at night. A Bronchoscopy/laryngoscopy is needed ASAP. This is potentially life threatening as a mucus plug could lead to obstruction.
Management: remove irritants (treat nasal/sinus disease/reflux – give promotility agent + gaviscon), remove caffeine, regular clear fluid every 20min. Then find therapists -SALT/physio who understand the upper airway. Encourage diaphragmatic breathing, and nasal predominant patterns. There are a few potentially useful drugs. Anecdotally – spiriva/atrovent seems to work better for upper airway than LABAs. Neuronal hypersensitivity is part of the pathophysiology, therefore amitryptilline may be effective. Botox to the larynx is better for laryngeal spasm than VCD (2/52 loss of voice, cough OK but reduced airway secretion protection).
There is a higher prevalence of psychopathology in people with BPD – this is likely compounded by trauma due to delays to diagnosis and recurrent trips to ED. SALT usually have training in psych assessments in voice problems so are well placed to assess.
By Dr James Hull (Training day at UCLH) RESPNet
